Creighton University Patient Demographic Form 2005-2026 free printable template
Show details
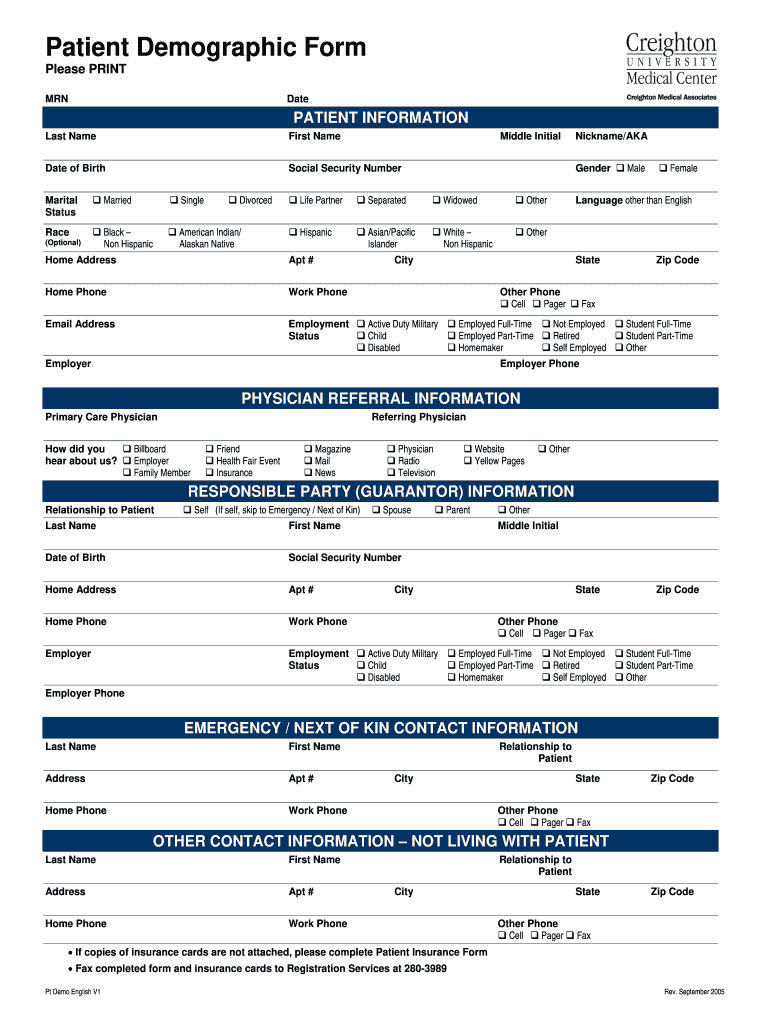
Patient Demographic Form Please PRINT MRN Date Last Name First Name Date of Birth Social Security Number PATIENT INFORMATION Marital Status Married Single Race Black Non Hispanic American Indian/ Alaskan Native Optional Divorced Middle Initial Gender Life Partner Separated Widowed Other Asian/Pacific Islander White Male Female Home Address Apt Home Phone Work Phone Email Address Nickname/AKA Language other than English City Employment State Other Phone Cell Pager Active Duty Military Child...
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign demographic form
Edit your demographic sheet form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your patient demographic form pdf form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing demographics form online



Use the instructions below to start using our professional PDF editor:
1
Check your account. In case you're new, it's time to start your free trial.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit patient demographic form. Rearrange and rotate pages, add and edit text, and use additional tools. To save changes and return to your Dashboard, click Done. The Documents tab allows you to merge, divide, lock, or unlock files.
4
Get your file. Select your file from the documents list and pick your export method. You may save it as a PDF, email it, or upload it to the cloud.
With pdfFiller, dealing with documents is always straightforward. Try it now!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out demographics sheet form
How to fill out Creighton University Patient Demographic Form
01
Begin by entering the patient's full name in the designated field.
02
Fill in the date of birth, ensuring the format matches the specified instructions.
03
Provide the patient's contact information, including address, phone number, and email.
04
Indicate the patient's gender and preferred pronouns if applicable.
05
Fill out the insurance information, including the provider's name and policy number.
06
Specify the patient's emergency contact details, including name and phone number.
07
Review the form for accuracy and completeness.
08
Sign and date the form if required.
Who needs Creighton University Patient Demographic Form?
01
Patients seeking medical services at Creighton University.
02
New patients who need to register with the healthcare facilities.
03
Anyone updating their personal information in the Creighton University health system.
04
Individuals required to provide demographic information for insurance purposes.
Fill
patient demographics examples
: Try Risk Free
People Also Ask about demographic form template
What are demographics in NHS?
The Personal Demographics Service (PDS) is the national electronic database of NHS patient details such as name, address, date of birth and NHS Number, which includes demographic information.
What is a demographic example?
Demographic information examples include: age, race, ethnicity, gender, marital status, income, education, and employment. You can easily and effectively collect these types of information with survey questions.
What is the demographic form?
The Individual Demographic Form (IDF) is designed to help users maintain essential information such as race, religion, SSN, Medicare, Medicaid number, admission date, program enrollment date, contacts, etc.
What is patient demographic?
Patient demographic data refers to all of the non-clinical data about a patient, including: name, date of birth, address, phone number, email address, sex, race, etc.
How do you write a demographic profile of a patient?
Patient demographics almost always include the following information: Full legal name. Date of birth. Biological sex. Gender. Contact information, including address. Ethnicity. Race.
What is the medical definition for demographics?
Medical demography is the application of demographic concepts, models, and techniques to the analysis of the dynamics of morbidity and mortality at all ages. The consequences of health, sickness, accidents, disability, and death for the size, composition, and structure of the population are projected.
Our user reviews speak for themselves
Read more or give pdfFiller a try to experience the benefits for yourself
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I modify my printable patient demographic form in Gmail?
In your inbox, you may use pdfFiller's add-on for Gmail to generate, modify, fill out, and eSign your demographic forms and any other papers you receive, all without leaving the program. Install pdfFiller for Gmail from the Google Workspace Marketplace by visiting this link. Take away the need for time-consuming procedures and handle your papers and eSignatures with ease.
How do I edit demographic page straight from my smartphone?
The pdfFiller mobile applications for iOS and Android are the easiest way to edit documents on the go. You may get them from the Apple Store and Google Play. More info about the applications here. Install and log in to edit example of patient demographics.
How do I fill out demographic form sample on an Android device?
Complete your patient demographics form and other papers on your Android device by using the pdfFiller mobile app. The program includes all of the necessary document management tools, such as editing content, eSigning, annotating, sharing files, and so on. You will be able to view your papers at any time as long as you have an internet connection.
What is Creighton University Patient Demographic Form?
The Creighton University Patient Demographic Form is a document used to collect essential information about patients for record-keeping, billing, and healthcare purposes within the university's health care system.
Who is required to file Creighton University Patient Demographic Form?
Patients receiving care at Creighton University Health services are required to file the Patient Demographic Form prior to or during their first visit.
How to fill out Creighton University Patient Demographic Form?
To fill out the Creighton University Patient Demographic Form, patients should provide accurate personal details including their name, contact information, date of birth, insurance information, and emergency contact details. It is important to complete all required fields and review the information for accuracy.
What is the purpose of Creighton University Patient Demographic Form?
The purpose of the Creighton University Patient Demographic Form is to gather necessary patient information that facilitates effective communication, healthcare delivery, billing, and compliance with legal and insurance requirements.
What information must be reported on Creighton University Patient Demographic Form?
The information that must be reported on the Creighton University Patient Demographic Form includes the patient's full name, date of birth, address, contact number, insurance details, and emergency contact information.
Fill out your Creighton University Patient Demographic Form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Patient Demographic Information is not the form you're looking for?Search for another form here.
Keywords relevant to patient demographics sheet
Related to demographic sheet template





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
