Creighton University Patient Demographic Form 2005-2024 free printable template
Show details
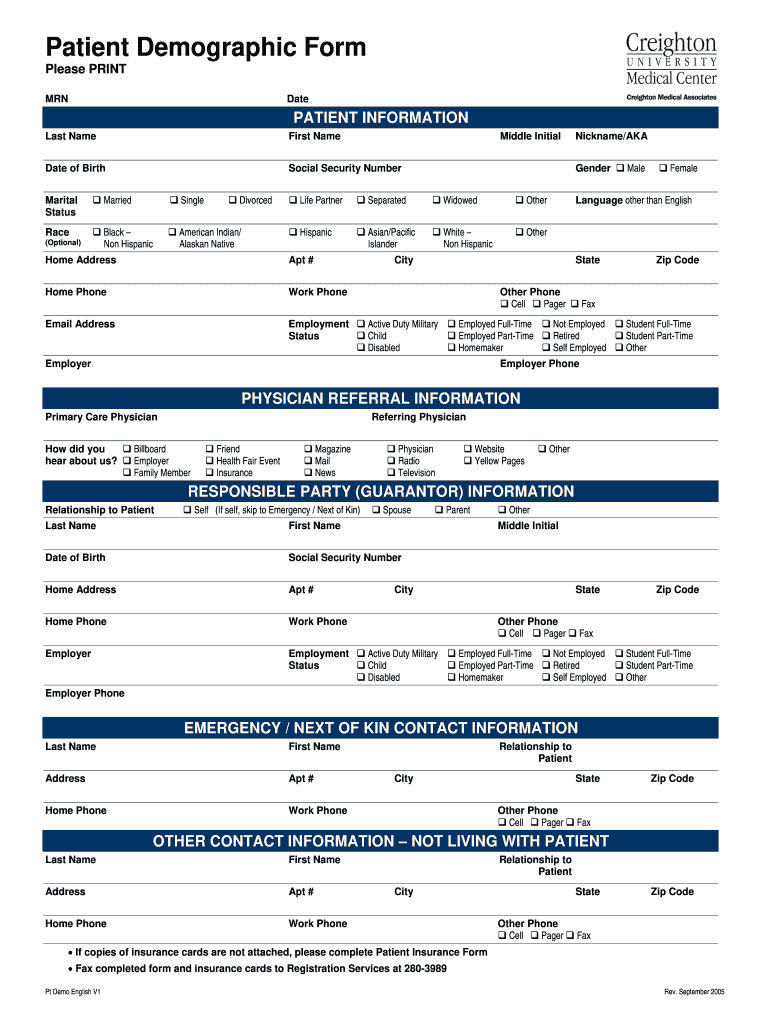
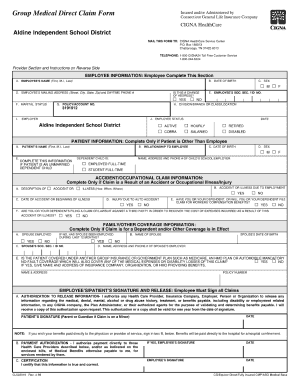
Patient Demographic Form Please PRINT MRN Date Last Name First Name Date of Birth Social Security Number PATIENT INFORMATION Marital Status Married Single Race Black Non Hispanic American Indian/ Alaskan Native Optional Divorced Middle Initial Gender Life Partner Separated Widowed Other Asian/Pacific Islander White Male Female Home Address Apt Home Phone Work Phone Email Address Nickname/AKA Language other than English City Employment State Other Phone Cell Pager Active Duty Military Child...
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign

Edit your patient demographic form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.

Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.

Share your form instantly
Email, fax, or share your patient demographic form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing patient demographic form online



Use the instructions below to start using our professional PDF editor:
1
Check your account. In case you're new, it's time to start your free trial.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit demographic form. Rearrange and rotate pages, add and edit text, and use additional tools. To save changes and return to your Dashboard, click Done. The Documents tab allows you to merge, divide, lock, or unlock files.
4
Get your file. Select your file from the documents list and pick your export method. You may save it as a PDF, email it, or upload it to the cloud.
With pdfFiller, dealing with documents is always straightforward. Try it now!
How to fill out patient demographic form

How to fill out a patient demographic form:
01
Begin by providing your personal information such as your full name, date of birth, and gender.
02
Next, fill in your contact details including your address, phone number, and email address.
03
Provide your insurance information, including the name of your insurance provider and your policy number.
04
Indicate your emergency contact information, including the name, phone number, and relationship of the person to contact in case of emergency.
05
If applicable, provide your primary care physician's name and contact information.
06
Specify any known allergies or medical conditions that may be relevant.
07
Sign and date the form to verify the accuracy of the information provided.
Who needs a patient demographic form:
01
Healthcare facilities and hospitals require patient demographic forms to maintain accurate and up-to-date records of their patients.
02
Physicians and medical professionals use these forms to gather essential information about their patients before providing appropriate healthcare services.
03
Insurance companies may also require patient demographic forms to process claims and verify eligibility for coverage.
Video instructions and help with filling out and completing patient demographic form
Instructions and Help about patient demographic form blank
Fill demographics form : Try Risk Free
People Also Ask about patient demographic form
What are demographics in NHS?
What is a demographic example?
What is the demographic form?
What is patient demographic?
How do you write a demographic profile of a patient?
What is the medical definition for demographics?
Our user reviews speak for themselves
Read more or give pdfFiller a try to experience the benefits for yourself
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is patient demographic form?
A patient demographic form is a document that collects and stores information about a patient's personal information and health history. It typically includes details such as name, address, date of birth, phone number, occupation, ethnicity, insurance information, and emergency contact. The form is used by healthcare providers to collect necessary information to provide treatment or services.
Who is required to file patient demographic form?
All healthcare providers are required to file patient demographic forms. It is typically completed by a healthcare professional, such as a doctor, nurse, or other healthcare provider, when a patient visits a medical facility. The form collects important information about the patient, such as name, address, age, gender, and insurance information.
How to fill out patient demographic form?
1. Start by filling in general patient information such as name, date of birth, address, and phone number.
2. Indicate the patient’s gender, marital status, and if they have any dependents.
3. Provide the patient’s insurance information, including the policy number and group number.
4. List the patient’s primary care physician and their contact information.
5. Indicate the patient’s race, ethnicity, and primary language.
6. Provide any additional information that may be required, such as a list of current medications, medical conditions, and allergies.
7. Have the patient sign and date the form to confirm that the information is correct.
What is the purpose of patient demographic form?
The purpose of a patient demographic form is to collect basic information about a patient. This information is used to create a patient profile, which is used to identify the patient and track their medical history. It may also be used to provide information to medical staff to ensure they are able to adequately provide care.
What information must be reported on patient demographic form?
The information that must be reported on a patient demographic form typically includes:
1. Full name: First name, middle name (if applicable), and last name of the patient.
2. Gender: Male, female, or other (if applicable).
3. Date of birth: The patient's date of birth in the format of month/day/year.
4. Address: The residential address of the patient, including street name, city, state, and zip code.
5. Phone number: Contact number of the patient or their primary contact.
6. Email address: The patient's email address (optional).
7. Emergency contact: Name and phone number of a person to be contacted in case of emergency.
8. Insurance information: Name of the insurance provider, policy number, and group number (if applicable).
9. Preferred language: Language preference of the patient for communication.
10. Ethnicity: The patient's ethnic background, which may include options like Caucasian, African-American, Hispanic, Asian, etc.
11. Race: The patient's racial background, typically categorized as White, Black or African American, Asian, Native American, Hawaiian or Pacific Islander, or other.
12. Marital status: The patient's marital status - single, married, divorced, widowed, etc. (optional).
13. Occupation: The patient's current or previous occupation (optional).
These are common details that may be required on a patient demographic form, but the exact information may vary depending on the healthcare facility and their specific requirements.
What is the penalty for the late filing of patient demographic form?
The penalty for the late filing of a patient demographic form may vary depending on the specific regulations and policies of the healthcare facility or organization handling the form. In general, there may not be a direct financial penalty for the late filing of a patient demographic form, but it can potentially result in administrative consequences or delays in processing the information. These consequences may include:
1. Delays in accessing medical care: Late filing of the patient demographic form may result in delays in processing the necessary paperwork, which can in turn affect the patient's ability to receive timely medical care.
2. Inaccurate medical records: Failing to provide accurate demographic information promptly can lead to errors in the patient's medical records. This can impact the quality of care delivered and potentially result in complications or misdiagnoses.
3. Billing and insurance issues: Late filing or incomplete patient demographic information can cause problems with billing and insurance claims. It may result in delayed or denied reimbursement for medical services, leading to financial difficulties for both the patient and the healthcare provider.
It is vital for healthcare facilities and organizations to have prompt and accurate patient demographic information to provide efficient and effective care. Therefore, it is generally encouraged to file the patient demographic form in a timely manner to avoid any potential negative consequences.
How do I modify my patient demographic form in Gmail?
In your inbox, you may use pdfFiller's add-on for Gmail to generate, modify, fill out, and eSign your demographic form and any other papers you receive, all without leaving the program. Install pdfFiller for Gmail from the Google Workspace Marketplace by visiting this link. Take away the need for time-consuming procedures and handle your papers and eSignatures with ease.
How do I edit printable patient demographic form straight from my smartphone?
The pdfFiller mobile applications for iOS and Android are the easiest way to edit documents on the go. You may get them from the Apple Store and Google Play. More info about the applications here. Install and log in to edit demographic sheet medical.
How do I fill out patient demographics template on an Android device?
Complete your patient demographic form pdf and other papers on your Android device by using the pdfFiller mobile app. The program includes all of the necessary document management tools, such as editing content, eSigning, annotating, sharing files, and so on. You will be able to view your papers at any time as long as you have an internet connection.
Fill out your patient demographic form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Printable Patient Demographic Form is not the form you're looking for?Search for another form here.
Keywords relevant to patient demographic sheet form
Related to medical demographic form


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
